Case Report: Use of BIO-C Repair – a bioceramic based cement – in the endodontic retreatment in teeth with open apex
BIO-C® Repair | Angelus
Lupicínio Moraes dos Santos
Prof. Clauber Romagnoli
Prof. Douglas G. N. Cortez
Prof. Renato Interliche
Introduction
Teeth requiring endodontic retreatment always present a challenge for the clinician. However, teeth indicated for retreatment that have incomplete rhizogenesis are even more challenging.
Teeth in this situation do not have apical constriction, which functions as a natural barrier to contain the filling material inside the root canals. It is therefore more difficult to maintain the root canal filling within the desired limits.
There are some alternatives for these situations that can prevent the overextension of the endodontic filling, such as the apexification technique, where intracanal medication changes are applied with calcium hydroxide until an apical cementum barrier is formed that will function to contain the root canal filling material (Pereira et al., 2021).
Another option is the manufacture of an apical plug with materials suitable for this purpose. For this method, MTA has been exemplified as the material of choice (Steinig, Regan, Gutmann, 2003).
Finally, regenerative endodontic therapy also appears as a possible approach to these cases. In this case, there is no need to contain the material inside the canal, as the blood clot will be the material that will fill the root canal (Banchs e Trope, 2004).
A material that can be utilized for this purpose is Bio-C Repair (Angelus, Londrina, Brazil). This bioceramic-based cement is recommended for several clinical situations due to its biocompatibility, hard consistency, ease of handling and ready-to-use characteristics. It is commercially available in syringes to facilitate quick and simple use.
The aim of this case report is to describe a clinical case where Bio-C Repair was used not only as an apical plug but also as a root canal filling material in an endodontic retreatment of an element with an apical lesion and open apex.
Case report
L.H.G., 29 years old, was admitted to the clinic for evaluation and treatment of tooth 11 (right maxillary central incisor), which showed darkening of the crown.
The evaluated tooth had a slight chromatic alteration and the patient reported trauma in the region, but it was not clear how long ago this had occurred.
The patient reported that the tooth had already been endodontically treated at the time of the accident.
At the time of the clinical examination, he did not present pain, fistula, or any other sign/symptom.
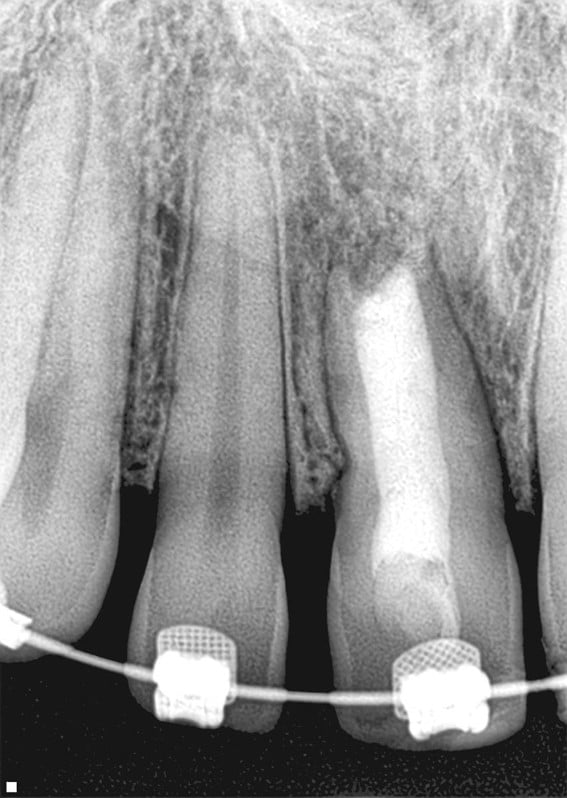
Through the radiographic examination, an insufficient root canal filling was observed, presenting an image suggestive of a periapical lesion (Figure 1).

The details shown in radiograph were explained to the patient and the suggested treatment plan was non-surgical endodontic retreatment followed by tooth bleaching.
In the following session, anesthesia, conventional coronary access, and absolute isolation were applied.
Subsequently, the filling material was removed from the root canal with the aid of manual files, Gates-Glidden drills and rotary files until the complete cleaning of the root canal was verified radiographically (Figure 2).

During this step, sodium hypochlorite (2.5%) was used as an irrigating solution between each instrument change in a volume of at least 2 ml in each application.
The canal working length was verified radiographically (Figure 3).

After the canal was completely unfilled, passive ultrasonic irrigation (PUI) was performed in three alternating 20 second cycles of sodium hypochlorite and 17% EDTA, aiming for the complete removal of the smear layer. For this, the Irrisonic insert (Helse ultrasonic, Ribeirão Preto, Brazil) was utilized in an ultrasonic unit.
At the end of this step, with the same ultrasound insert, continuous ultrasonic irrigation (CUI) was performed to remove the remaining irrigant solutions with a saline solution that was previously connected to the ultrasonic unit.
After removing the excess of saline solution with aspiration and an absorbent paper cone, a small amount of Bio-C Repair was inserted into the canal to form the apical plug. This material was accommodated in the region with a large-diameter endodontic tamper, as the diameter of the canal was quite wide.
With the apical plug completed, we observed that the length of the canal that still needed to be filled was small, which led us to change the canal filling strategy. We continued with the complete root canal filling with increments of Bio-C Repair up to the cervical third, which was confirmed radiographically during the transoperative period (Figure 4).

The pulp chamber cavity was cleaned and sealed with composite resin. No medication was administered, except prescribing the use of analgesics if necessary.
The patient returned for a follow-up appointment thirty days after the end of the procedure and did not report pain, swelling, or discomfort (Figure 5).
A follow-up was performed two and a half years later (Figure 6), in which a very favorable periapical situation can be observed. No fistula was detected and the patient did not report any complications during this period.

Discussion
Two important points of the difficulties for endodontic treatment or retreatment of teeth with open apexes are canal decontamination and filling.
The reduction of intracanal microbiota is carried out in these cases mainly by the action of the irrigating solution. As teeth with an incomplete apex normally have thin dentin walls, vigorous instrumentation is not indicated, leaving the responsibility for eliminating the largest number of bacteria to the irrigating solutions and intracanal medication.
The root canal filling presents the difficulty of containing the filling material (sealer and gutta-percha cones) within the canal itself since there is no apical constriction that physically prevents this material from entering the periapex.
For this last reason, specific techniques are used to avoid overextension of the filling material, such as the apexification technique, apical plugs, and revascularization.
In this case report, revascularization was not chosen due to the future possibility of installing a prosthesis with the consequent installation of intraradicular posts for prosthesis retention.
The apexification technique was also discarded, because of the long time it takes to perform it (Zenkner, Pagliarin, Barletta, 2009).
Consequently, we looked for an alternative that would be quick to apply and allow us to recover the periapical tissues and also permit the installation of a post and prosthesis in the future, if necessary (Niedermaier, Guerisoli, 2013).
The apical plug technique was carried out and, given the small size of the root, the canal was not filled with conventional gutta-percha cones and sealer. After completing the apical plug, a small extension of the root was left unfilled and this led us to choose to fill the rest of the canal with Bio-C Repair cement. This bioceramic-based cement, as it has an excellent sealing capacity, also worked as a cervical plug to contain the internal tooth bleaching material, thus performing two functions: apical and cervical plug.
At the follow-up appointment two and a half years later, we observed an excellent apical and periodontal condition. We saw that the periapical situation was normal and the patient did not report any pain or other complications, such as pain or swelling.
Therefore, we can see that this bioceramic-based repair cement was sufficient for the resolution of the root canal filling phase in a tooth where the apex was open, preventing material extrusion beyond the apex and providing conditions for recovery of periapical tissues.
Conclusion
We conclude, based on the described clinical case, that the Bio-C Repair material is a very viable alternative for the root canal filling of teeth that present an open apex, whether for making an apical plug or filling the canal in cases of short roots.
References
Banchs F, Trope M. Revascularization of immature permanent teeth with apical periodontitis: new treatment protocol? J Endod, V. 30, p. 196–200, 2004.
NIEDERMAIER, Katherynn; GUERISOLI, Danilo. Apicificação com plug apical de MTA em dente traumatizado. Revista Brasileira de Odontologia. v.70, n.2, p.213-215. 2013.
PEREIRA, Helen; NASCIMENTO, Joyce; LOBATO, Carina; BRASIL, Mariana; GOES, Silas; MEIRA, Gabriela; LOPES, Luana; SILVA, André. Tratamento endodôntico em dente com rizogênese incompleta com a utilização do hidróxido de cálcio: Relato de caso. Research, Society and Development. v.10, n.16, p.1-9. 2021
Steinig TH, Regan JD, Gutmann JL. The use and predictable placement of mineral trioxide aggregate in one-visit apexification cases. Australian Endodontic Journal. V. 29, p. 34–42, 2003
WHITHERSPOON, David. Vital Pulp therapy with new materials: New directions and treatment perspectives – permanente teeth. Journal of endodontics. v.34, n.7, p. 25-28. 2008.
ZENKNER, Clacir; PAGLIARIN, Claudia; BARLETTA, Fernando. Apicificação de incisivos centrais superiores usando hidróxido de cálcio: Relato. Revista Saúde (Santa Maria). v.35, n.1, p.16-20. 2009.
Produtos em destaque

NEW!
BIO-C® REPAIR Monodose
Bioceramic reparative material ready to use: The ideal dose for clinical practice


 Materiais Informativos
Materiais Informativos
Acesse bula, catálogo, perfil técnico e trilhas de conhecimento para saber mais sobre nossos produtos!
Leia também
Nenhum caso clínico encontrado 😅
SAC
Specialized Customer Service
Monday to Friday, from 7:30 a.m to 5:30 p.m (GMT-3).