Use of MTA-FILLAPEX and BIO-C SEALER endodontic sealers in pulp necrosis
Bioceramics | Angelus
Clauber Romagnoli, specialist in endodontics and implantology; master in Endodontics
Douglas Giordani Negreiros Cortez, specialist in endodontics and implantology; master and doctor in Endodontics
Renato Interliche, specialist in endodontics and implantology; master in Endodontics
Abstract
The aim of this study is to report a clinical case performed during an endodontic specialization course, in which two teeth were endodontically treated and filled with two different endodontic sealers. After completion of the treatment, a radiographic and clinical control of the case was performed after three and a half years. Based on the results obtained, we conclude that the endodontic treatment of the two teeth was satisfactory.
Introduction
Apical periodontitis may develop asymptomatically and be detected only by routine radiographic examinations in the dental clinic (NEVILLE, 1998; SOUZA, et al., 2003).
In some cases, fistulas or edema are observed in the periapical region, suggesting the presence of endodontic problems in the teeth being examined. A change in the color of the dental crown is also a clinical sign of endodontic problems.
Teeth with extensive fractures or deep caries are also commonly associated with asymptomatic chronic apical periodontitis. Non-surgical endodontic treatment and restoration of dental prostheses are suggested as the first alternative for the treatment of these cases, as needed. With a very high success rate, this option proves to be fast in most cases and prevents tooth loss.
To this end, various materials and techniques for endodontic treatment have been developed, including a variety of new dental materials that have entered the market with a very favorable clinical success rate. Among these materials, endodontic sealers are extremely important for the process of root canal filling.
The aim of this study is to report a clinical case in which the endodontic treatment of two teeth of the same patient was performed with two different endodontic sealers.
Case report
In March 2019, a 39-year-old female patient (M.P.) attended an appointment at the dental clinic of Educação Inteligente School (Ei Uningá, Londrina, PR, Brazil) for the evaluation of teeth 34 and 35.
On clinical examination, both teeth were found to have extensive coronal destruction and an unsatisfactory provisional restoration (35), but no spontaneous pain was present.
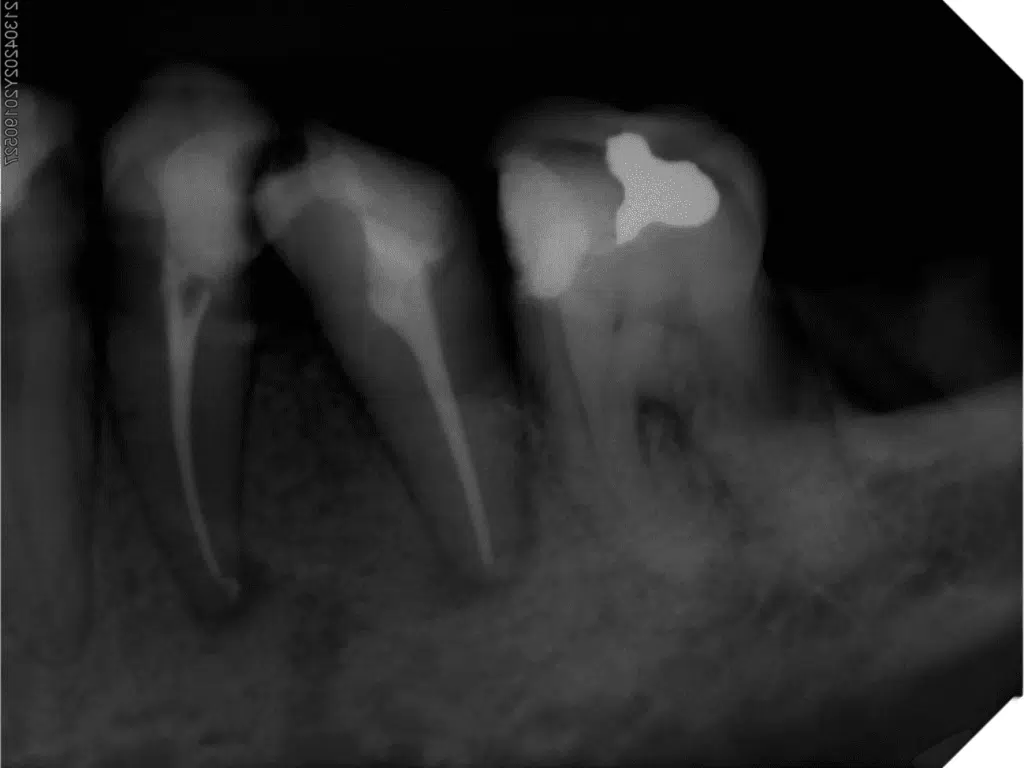
Initial radiographic examination revealed extensive caries on teeth 34 and 35 (Figure 1).

After radiographic and clinical examinations, the patient was informed that endodontic and prosthetic treatment would be required to rehabilitate both tooth elements.
After discussing the proposed treatment with the patient, she agreed to begin endodontic treatment.
Both teeth underwent the same endodontic treatment sequence: conventional endodontic access and removal of all carious tissue, absolute isolation, and initial exploration with a #10 K-File to perform disinfecting penetration and irrigation with 2.5% sodium hypochlorite solution between file changes.
The biomechanical preparation of the root canal was performed according to the preparation technique suggested by the Londrina Endodontics team (see below):
- Cervical preparation with a #15./05 rotary file or up to 2/3 of the apparent length of the root canal
- Performing patency with #25./01 rotary files at 1 mm beyond the apparent length of the tooth on the radiograph
- Electronic working length determination
- Instrumentation with the #15./05 rotary file at working length
- Instrumentation with the #25./05 rotary file at working length
- Instrumentation with the #40./05 rotary file at working length
- Passive Ultrasonic Irrigation using an Irrisonic ultrasonic insert (Helse ultrasonic, Ribeirão Preto, Brazil) (Passive ultrasonic irrigation) with irrigating solutions EDTA (17%) and NaOCl (2.5%).
After these steps, the canal was dried with absorbent paper points and filled with using the hydraulic compression technique (with a gutta-percha single cone), changing only the root canal sealers used.
Bio-C Sealer, a bioceramic-based sealer (Angelus, Londrina, Brazil), was used for tooth 34, and MTA-Fillapex Sealer (Angelus, Londrina, Brazil) was used for tooth 35.
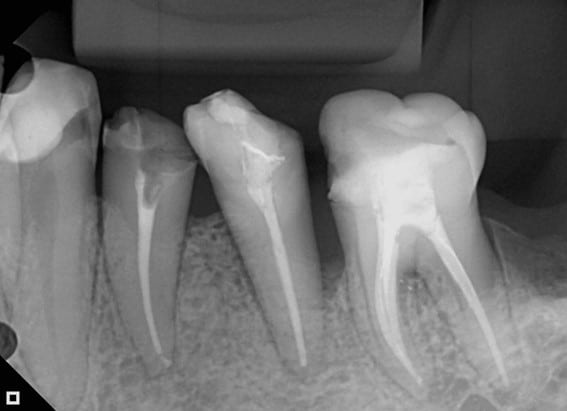
A radiograph was taken to verify the final quality of the root canal filling (Figure 2), and the patient was advised to attend a dental restoration course for the rehabilitation of the treated teeth.
Thirty days after the endodontic treatment was completed, the patient returned to the clinic for radiographic follow-up (Figure 3). At this time, she did not report any pain, swelling, or fistula in the region.

After completion of the endodontic treatments, the patient was advised to make an appointment at the specialization course in dental prosthesis at the same school to rehabilitate the teeth.
After three and a half years, the patient returned to the dental school for rehabilitation of the teeth, and at that time a control radiograph was taken to check the condition of the teeth before she was referred for rehabilitation (Figure 4).
Discussion
In this clinical case, we had the opportunity to evaluate, in the same individual, two different bioceramic-based endodontic sealers where the only variable was the root canal sealer used.
The two teeth were prepared and treated similarly by the same clinician (RI).
It was observed that in the three and a half year clinical radiographic control, tooth 34 was without coronal shielding, but did not show any apical repercussion of root canal contamination or the presence of fistula.
The full regression of the apical lesions of the two teeth and complete absence of any painful symptomatology was also verified. However, a periodontal pocket was evident on the distal side of element 35, probably resulting from food impaction due to non-rehabilitation of the tooth.
The success of endodontic therapy mainly depends on the decontamination of root canals. This is achieved during the biomechanical preparation of the canals, using intracanal medications and also by obturation of the root canal system.
The new endodontic sealers with bioceramic composition present bioactivity, which could positively impact the recovery of periapical lesions (HAN, OKIJI, 2013; LIMA, 2017).
Root canal fillings are responsible for trapping bacteria resistant to the preparation so that they are eliminated due to lack of nutrients. Obturation has the function of preventing recontamination of the canals, which was quite evident in this case, when we analyzed the absence of apical lesion in a tooth that had lost its cervical shielding (tooth 34).
As for the use of root canal sealers, we found that Bio-C Sealer was particularly convenient because it was premixed, which streamlined clinical care. However, given the experience we already have with MTA-FILLAPEX sealer, we can say that it is also very practical and offers the possibility of being used with self-mixing tips. In this case, MTA-FILLAPEX sealer was used in the paste-to-paste system, where the product in equal parts for use.
It is important to note that both of the root canal sealers used have excellent features for clinical use. Radiopacity, working time, flow and all the properties inherent to endodontic sealers proved to be satisfactory for the materials evaluated here (ROMAGNOLI et al., 2018; SANTOS, 2018).
Conclusion
Based on the development of this clinical case, we conclude, within the limitations of this case report, that the root canal sealers used are excellent options for non-surgical endodontic treatments.
References
BROON, N. J. et al. Respuesta inflamatoria de Bioceramic a la implantación de tubos de dentina en tejido subcutáneo de ratas. Revista Odontológica Mexicana, v. 20, n. 3, p. 174-178, 2016.
BUENO, C. R. E. et al. Biocompatibility and biomineralization assessment of bioceramic-, epoxy-, and calcium hydroxide-based sealers. Brazilian Oral Research, v. 30, n. 1, 2016.
CARVALHO, C. N. et al. Micropush-out dentin bond strength and bioactivity analysis of a bioceramic root canal sealer. Dental Materials, v. 29, p. e79, 2013.
HAN, L.; OKIJI, T. Bioactivity evaluation of three calcium silicate‐based endodontic materials. International Endodontic Journal, v. 46, n. 9, p. 808-814, 2013.
KOHLI, M. R. et al. Spectrophotometric analysis of coronal tooth discoloration induced by various bioceramic cements and other endodontic materials. Journal of Endodontics, v. 41, n. 11, p. 1862-1866, 2015.
LIMA, NFF et al. Cimentos biocerâmicos em endodontia: revisão de literatura. Revista da Faculdade de Odontologia-UPF, v. 22, n. 2, 2017.
NEVILLE, B.W. et al. Doenças da polpa e periápice. In: NEVILLE, B.W. et al. Patologia oral e maxilofacial. 1ªed. Rio de Janeiro: Guanabara Koogan, 1998. c.3, p. 93-119
LIU, S.; WANG, S.; DONG, Y. Evaluation of a bioceramic as a pulp capping agent in vitro and in vivo. Journal of Endodontics, v. 41, n. 5, p. 652-657, 2015.
MCMICHAEL, GE; PRIMUS, CM; OPPERMAN, LA. Dentinal tubule penetration of tricalcium silicate sealers. Journal of Endodontics, v. 42, n. 4, p. 632-636, 2016.
ROMAGNOLI C.; FELIZARDO, K.R.; GUIRALDO, R.D. et al. Evaluation of phisico-chemical and mechanical properties of MTA-based root canal sealer. Brazilian Journal of Oral Sciences, V. 17, p. 1-11, 2018.
SANTOS, J. L. Cimentos biocerâmicos: uma breve revisão bibliográfica e apresentação de casos clínicos. Monografia. Londrina – Brasil: Universidade do Norte do Paraná, 2018.
SOUZA, M.E. et al. Lesões periapicais: estudo epidemiológico. Rev Bras Patol Oral, v.2, n.1, p.30-34, 2003.
Produtos em destaque

NEW!
BIO-C® REPAIR Monodose
Bioceramic reparative material ready to use: The ideal dose for clinical practice


 Materiais Informativos
Materiais Informativos
Acesse bula, catálogo, perfil técnico e trilhas de conhecimento para saber mais sobre nossos produtos!
Leia também
Nenhum caso clínico encontrado 😅
SAC
Specialized Customer Service
Monday to Friday, from 7:30 a.m to 5:30 p.m (GMT-3).